
Compare FHIR and openEHR for urgent-care EHRs: FHIR for fast interoperability, openEHR for detailed clinical storage and workflows.
FHIR and openEHR serve different roles in healthcare IT, particularly when it comes to clinical workflows in EHR systems. Here's the essence:
| Feature | FHIR | openEHR |
|---|---|---|
| Purpose | Data exchange via APIs | Clinical data modeling & storage |
| Core Unit | Resources (e.g., Patient, Observation) | Archetypes & Compositions |
| Query Language | FHIRPath / FHIR Search | AQL (Archetype Query Language) |
| Regulation | Mandated in the U.S. | Voluntary adoption |
| Best Use Case | Interoperability | Longitudinal records, research |
If you're in urgent care, start with FHIR for compliance and quick wins. Add openEHR later for deeper clinical data management as your system grows.
FHIR vs. openEHR: Side-by-Side Comparison for Clinical Workflows
FHIR is a communication standard that leverages RESTful APIs and formats like JSON and XML. It operates on the "80/20 rule", meaning its base resources - such as Patient and Observation - cover most common scenarios. However, in practice, this balance often shifts to around 65/35, requiring more custom profiling to meet specific needs.
In urgent care scenarios, FHIR's API-driven approach shines. Imagine a patient arriving at an emergency room: clinicians can quickly retrieve critical information, such as medication history, recent lab results, or allergy details, from external systems. This capability is further enhanced by frameworks like SMART on FHIR and CDS Hooks, which enable seamless integration with labs, e-prescribing solutions, and payers.
That said, FHIR's ecosystem isn't without challenges. By 2026, it is expected to include 1,319 distinct packages from 602 projects across 53 jurisdictions. This "profile proliferation" can make system compatibility across different regions and health networks more complex.
While FHIR is excellent for fast data exchange, it isn't designed to handle the level of structured, detailed record-keeping that openEHR provides.
Unlike FHIR, openEHR prioritizes detailed data structuring and the integrity of long-term records. Its "two-level model" separates technical infrastructure from clinical knowledge, allowing clinicians - not just developers - to define data structures. These structures, called archetypes, are comprehensive datasets that capture all relevant clinical details from the start.
Take openEHR's blood pressure archetype as an example. It doesn't just log systolic and diastolic values; it also includes details like the patient's body position, the cuff size, and the measurement site. This level of detail enhances clinical accuracy and supports applications like research and AI training, which depend on consistent, structured data.
Another standout feature of openEHR is its focus on clinical governance. Digital health researcher Jishen Pfeiffer explains:
"The key insight [of openEHR]: clinical knowledge is separated from the software. A change in clinical best practice can be made in the archetype without rewriting the EHR software."
For instance, if a protocol for sepsis screening is updated, changes can be implemented at the archetype level without requiring database migrations or software overhauls.
Here’s a side-by-side look at how FHIR and openEHR differ:
| Feature | HL7 FHIR | openEHR |
|---|---|---|
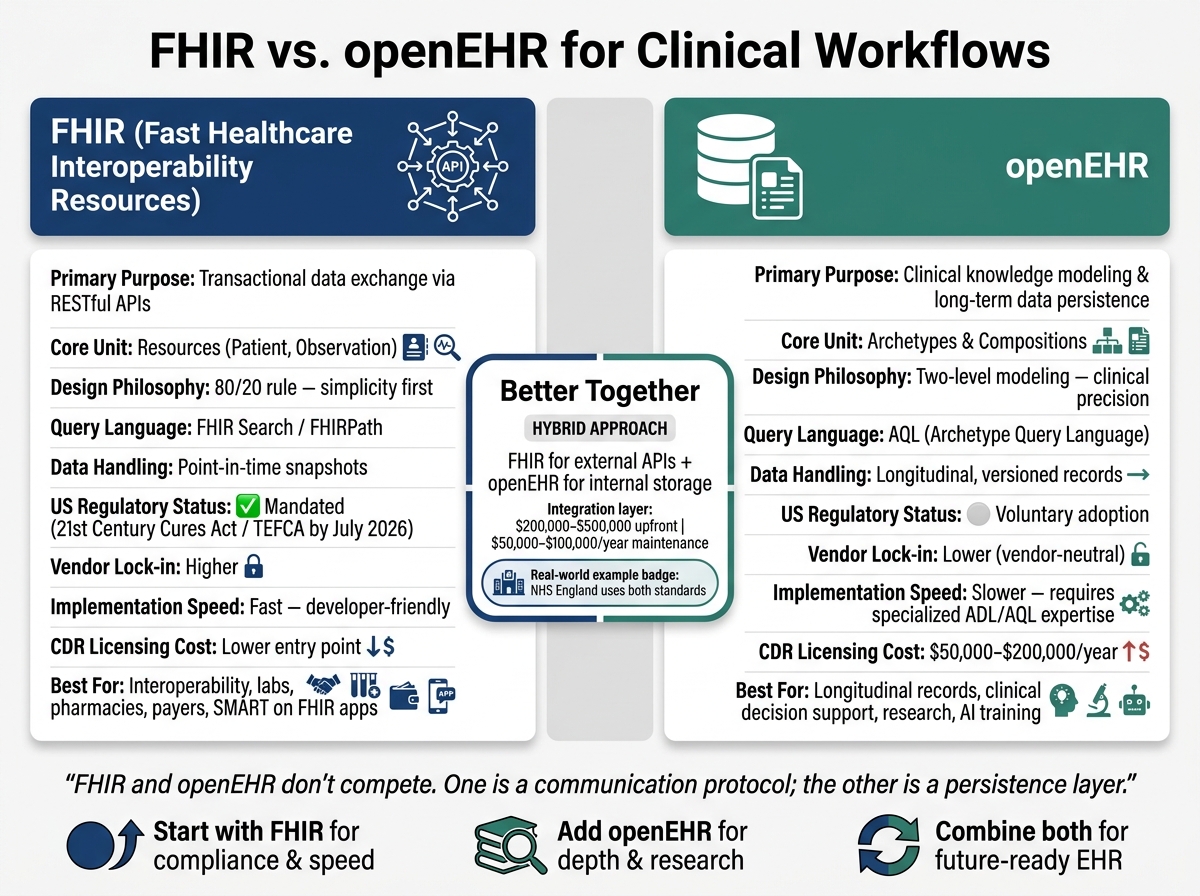
| Primary Purpose | Transactional data exchange (API) | Clinical knowledge modeling & persistence |
| Core Unit | Resources (Patient, Observation) | Archetypes & Compositions |
| Design Philosophy | 80/20 rule (simplicity first) | Two-level modeling (clinical precision) |
| Query Language | FHIR Search / FHIRPath | AQL (Archetype Query Language) |
| Data Handling | Point-in-time snapshots | Longitudinal, versioned records |
| Vendor Lock-in | Higher (proprietary internal models) | Lower (vendor-neutral persistence) |
| US Regulatory Mandate | Yes (21st Century Cures Act) | No (voluntary adoption) |
| Workflow Support | Real-time integration, patient-facing apps | Clinical decision support, research, AI |
Ultimately, these two standards address different needs in healthcare. As Yogesh Daga, Founder & CEO of Nirmitee, succinctly explains:
"FHIR and openEHR don't compete. They solve fundamentally different problems in the healthcare data lifecycle. One is a communication protocol; the other is a persistence layer."
FHIR's RESTful API is a powerful tool for streamlining urgent care workflows. Imagine a patient checking in - FHIR can instantly pull their medication history, allergies, and recent lab results from external systems, cutting out the need for manual searches.
Tools like CDS Hooks and SMART on FHIR take this further by embedding clinical decision support directly into the care process. These tools allow apps like imaging viewers, e-prescribing tools, or triage calculators to launch within the EHR using OAuth 2.0, making the workflow smoother and more efficient.
For situations where speed is critical, the FHIR Subscriptions Framework ensures real-time updates. Whenever a resource changes, notifications are pushed to downstream systems like lab queues or tracking boards. This eliminates the need for constant polling and can make a real difference in urgent care - where even a 10-minute delay in lab results could impact treatment decisions.
While FHIR excels at data exchange, openEHR shines in modeling clinical workflows. Its Task Planning (TP) specification allows healthcare teams to create detailed, executable care pathways. These pathways include tasks, decision points, timing rules, and role assignments, all laid out as structured plans.
Take, for example, a sepsis screening pathway. Using openEHR Task Planning, the system can query the Clinical Data Repository (CDR) directly through AQL to check if serum lactate levels exceed 2 mmol/L. If they do, the workflow automatically advances to the next task. This kind of built-in awareness of clinical data and logic sets openEHR apart from generic workflow engines like BPMN, which require extra integration to access clinical data and lack features like medication timing or performer roles.
The impact of openEHR in real-world settings is clear. A hospital in Portugal used openEHR Task Planning to manage over 6,800 imaging exam requests, covering everything from capturing requests to assigning radiologists and delivering results. The result? Shorter patient waiting times and a complete audit trail, all stored as structured data in the CDR.
When combined, FHIR and openEHR create a robust solution for urgent care workflows. FHIR handles interoperability, while openEHR focuses on clinical data persistence and modeling.
"FHIR for interoperability, openEHR for clinical data modeling and storage. The question becomes: how do you connect them?" - Jitendra Choudhary, CTO & Co-Founder, Nirmitee
In urgent care, where fast data exchange and precise modeling are equally important, this combination ensures workflow integrity. One common approach is the FHIR Facade. Here, openEHR acts as the single source of truth in the CDR, while a translation layer converts FHIR queries into AQL and returns responses in FHIR format. This setup provides external systems with a standard FHIR API while maintaining full clinical precision internally.
A regional hospital network in Northern Germany demonstrated the effectiveness of this approach. By integrating three Clinical Data Repositories and two Hospital Information Systems using FHIR R4 and openEHR, they reduced sync latency to under 15 minutes (from hours of manual compilation) and achieved a 99.9%+ sync success rate. Oncologists could collaborate on treatment decisions using unified patient records, with structured tumor board decisions captured in a 20-field FHIR QuestionnaireResponse.
Platforms like Ottehr, built on FHIR R4, can act as the interoperability layer in such architectures. While Ottehr manages real-time data exchange, an openEHR CDR handles long-term clinical data storage and modeling.
One important consideration: reconciling terminology between FHIR ValueSets and openEHR archetype constraints often accounts for 40–60% of the transformation effort. It’s worth planning for this early in the process.
When deciding between FHIR and openEHR, the choice comes down to what each layer of your system needs. For urgent care settings, the most important factors are regulatory compliance, speed of implementation, clinical customization, and how well the system handles long-term data storage.
In the United States, compliance heavily favors FHIR. By July 2026, TEFCA mandates that systems expose FHIR APIs and meet USCDI v3 standards. In contrast, openEHR is not required by US regulations - it’s an optional architectural framework. If your practice needs to exchange data with insurers, labs, or national networks, FHIR is the default option.
FHIR also excels in implementation speed. Its REST-based design and large developer community make it easier to deploy quickly. On the other hand, openEHR demands expertise in Archetype Definition Language (ADL) and AQL, which can slow down initial setup. However, openEHR’s two-level modeling system allows clinicians to add new data fields without requiring database changes, offering greater adaptability over time.
Here’s a quick comparison of FHIR and openEHR based on key attributes:
| FHIR | openEHR | |
|---|---|---|
| Best for | Data exchange, regulatory compliance | Long-term clinical data storage and modeling |
| Implementation speed | Fast; developer-friendly REST APIs | Slower; requires specialized expertise |
| US regulatory status | Mandated by ONC/CMS/TEFCA | Voluntary |
| Clinical flexibility | Limited; relies on profiling and extensions | High; schema evolves without migrations |
| Query power | Multi-step FHIR searches often needed | Single AQL expressions for complex queries |
| Ecosystem size | Large; broad tooling and developer pool | Smaller; specialized talent required |
| Cost | Varies; FHIR-native platforms start at lower price points | CDR licensing: $50,000–$200,000/year |
Based on these factors, here’s how to decide which framework works best for your urgent care practice:
For most urgent care practices looking to grow over time, a dual-standard approach offers the best balance. Use FHIR for speedy external integration and regulatory compliance, and openEHR for robust internal data management. If budget or time is tight, start with FHIR - it delivers immediate value - then add an openEHR Clinical Data Repository (CDR) as your practice expands. Keep in mind that building a FHIR-to-openEHR transformation layer typically costs between $200,000 and $500,000, with annual maintenance running $50,000 to $100,000. Ongoing governance will likely require a part-time clinical informaticist.
FHIR and openEHR serve different purposes: FHIR focuses on moving data seamlessly between systems, while openEHR ensures clinical data is stored with precision and depth.
In the context of U.S. urgent care, FHIR is indispensable. With TEFCA requiring FHIR API exposure by July 5, 2026, it’s the go-to choice for quick integration with labs, pharmacies, and payers. If speed and interoperability are your top priorities, FHIR is the clear solution.
On the other hand, openEHR shines when managing longitudinal records, running advanced clinical queries, or supporting evolving clinical models. Its Archetype Query Language (AQL) simplifies complex clinical queries that could otherwise demand several chained FHIR searches.
For a robust and future-ready setup, combining both standards - FHIR for external APIs and openEHR for internal storage - offers the best of both worlds. NHS England has already adopted this dual-standard approach, pairing FHIR UK Core profiles for external data exchange with openEHR-based repositories for comprehensive patient records. However, this approach comes with a hefty price tag: initial costs range from $200,000 to $500,000, with annual maintenance costs between $50,000 and $100,000. Despite the expense, this hybrid model ensures regulatory compliance while maintaining the depth needed for clinical data management.
If resources or deadlines are tight, starting with FHIR is a practical choice, allowing room to expand your architecture later. This strategy underscores the importance of leveraging the strengths of each framework to create efficient, compliant, and scalable EHR workflows.
FHIR and openEHR work best when seen as complementary tools. FHIR excels at data exchange - think real-time communication, app integration, and sharing data at specific moments. On the other hand, openEHR is ideal for internal storage, handling structured and evolving clinical records, tracking patient histories over time, and managing complex queries. Many systems successfully combine the two: using openEHR for storing and organizing data, while relying on FHIR for access and seamless interoperability.
The simplest way to handle this is by using a FHIR facade layer. This layer takes FHIR REST API calls and converts them into Archetype Query Language (AQL) queries, which are compatible with an openEHR database. For write operations, it translates FHIR resources into openEHR compositions. Tools such as EHRbase FHIR Bridge or the openFHIR engine make this process smoother, allowing external applications to interact effortlessly while maintaining openEHR's clinical modeling structure.
The main difficulty in aligning FHIR with openEHR stems from their fundamentally different designs. FHIR is built around an API-driven, resource-based framework aimed at enabling flexible data exchange. On the other hand, openEHR prioritizes structured, long-term clinical data management through the use of archetypes. This contrast means bridging the gap often involves balancing FHIR’s straightforwardness with openEHR’s detailed semantic structure, as each system serves different purposes rather than being directly interchangeable.
